
|
MEGAOESOPHAGUS (Also been called chalasia,
achalasia, megalo-oesophagus, oesophageal paralysis)
Note for Pet Owners: This information is provided by
Provet for educational purposes only.
You should seek the advice of
your veterinarian if your pet is ill as only he or she can correctly advise
on the diagnosis and recommend the treatment that is most appropriate for
your pet.
Topics on this Page:
|
Description
Megaoesophagus means dilation of the oesophagus (gullet). This can be identified on plain (survey) Xrays or on contrast radiography - particularly following a barium swallow.
Cause
There are many potential causes of megaoesophagus including congenital abnormalities which may or may not be hereditary, neuromuscular disorders, obstructions of the oesophagus ( e.g. foreign bodies, vascular rings, cancer), toxic causes (e.g. lead ) and others (e.g. hypothyroidism, Addisons disease) . Persistent right aortic arch is a common congenital vascular ring abnormality which occurs at the base of the heart, and has been confirmed to be inherited in the German Shepherd Dog
is not now thought to be a common cause of idiopathic megaoesophagus in animals and as yet unidentified disorders of the neuromuscular system are thought to be the most likely cause in most cases. This is based upon the observation that loss of motor function is definitely present.Causes of secondary megaoesophagus include any condition which can interfere with neuromuscular function (e.g. myositis, myopathy, neuromuscular transmission, neuropathies.
Breed Occurrence
Megaoesophagus is the main cause of regurgitation in both dogs and cats. In veterinary referral centres about 1/1000 cases has this condition.
In young animals idiopathic megaoesophagus is known to be inherited * in Wirehaired Fox Terriers (simple autosomal recessive) and in Miniature Schnauzers (simple autosomal dominant or 60% penetrance autosomal recessive).
The following Breeds are predisposed to develop idiopathic megaoesophagus at an early age, and the condition may be congenital and/or genetically inherited* :
German Shepherd Dogs, Great Danes, Greyhounds, Newfoundlands, and
Abyssinian and Siamese Cats
Age
There are two distinct forms of megaoesophagus separated by age :
- Congenital megaoesophagus - present at birth and identified soon after weaning
- Acquired megaoesophagus - can develop at any age, due to a variety of causes.
Signs
Complications
In cases with inhalation, coughing
or dyspnoea
Diagnosis
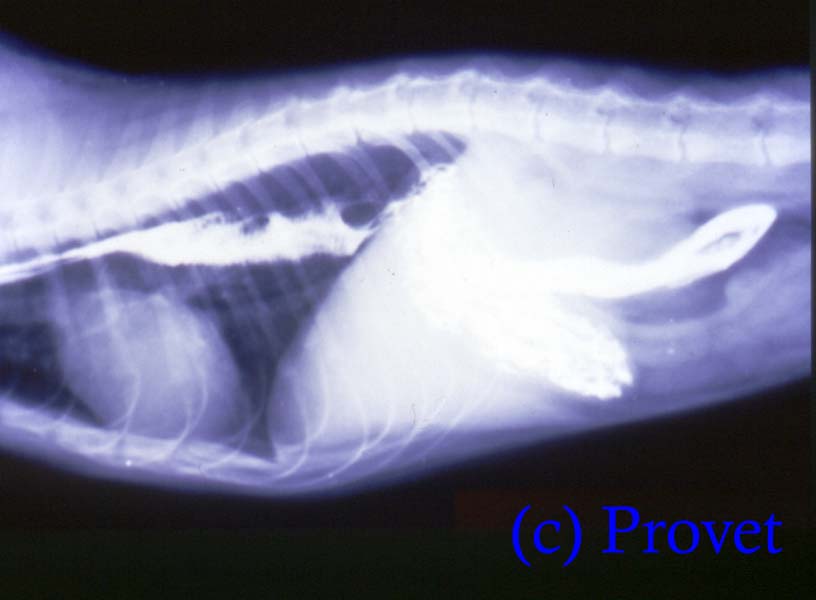
Xrays to confirm the presence of a dilated oesophagus, and in some cases for evidence of secondary inhalation of food material. Dilation of the oesophagus with air or food material can be seen on plain radiographs
The plain Xray below shows food accumulation in the oesophagus, with dilation due to air, and displacement of the wind-pipe (trachea) which is pushed down (ventrally) by the large oesophagus.

The use of contrast studies is very helpful to clearly demarcate the inner lining of the walls from the lumen contents and surrounding soft tissue structures.
Positive contrast material (such as barium or iodine preparations show up on XRay images as solid white. Negative contrast materials such as air or other gases show up as black.In megaoesophagus contrast materials eg a barium swallow are retained in the oesophagus.
The XRay below shows white contrast material (barium) retained in the oesophagus
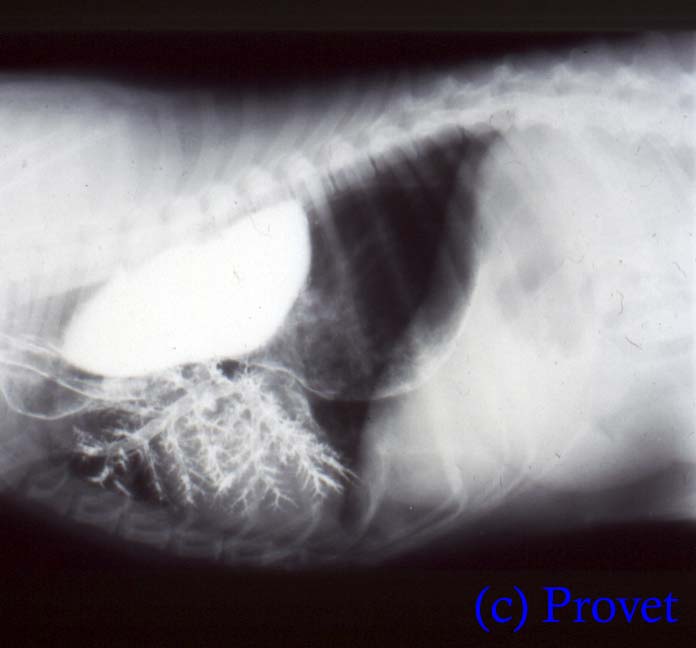
In the XRay below liquid barium has been given and, following regurgitation it has been inhaled into the lungs giving a clear outline of both the oesophagus and the bronchial tree (called a bronchogram when performed deliberately).. This clearly indicates the functional difficulties that these patients have when swallowing liquids and foods.
Passing an endoscope down the oesophagus is a useful diagnostic tool to identify and in some case remove obstructions in the lumen (intralumenal) or oesophageal wall (intramural).
Image intensification demonstrates abnormal peristaltic waves with asynchronous activity in the caudal segment of the oesophagus.
Treatment
Secondary megaoesophagus - treat the underlying cause e.g. ligate and section constricting vascular rings (e.g. persistent right aortic arch)
Metoclopramide might help as it encourages oesophageal contractions in the distal segment, and calcium channel blockers (e.g. nifedipine) might prove useful. Antibiotics are used to treat aspiration pneumonia. Cutting the muscular wall of the oesophagus (myotomy) may be useful in some cases though it does not improve oesophageal function.
Prognosis
Long term problems
Updated October 2013
d>